
What’s Actually Changing During Perimenopause
Perimenopause is often framed as a period of decline—but physiologically, it’s better understood as a phase of increasing variability.
The systems responsible for metabolism, recovery, and body composition don’t stop working. What changes is how consistently they respond. When you understand this shift, it becomes easier to adjust your approach—rather than abandoning what works or doubling down in the wrong direction.
A Shift in Hormonal Consistency — Not Immediate Loss
Perimenopause typically begins in the late 30s to mid-40s, though timing varies.
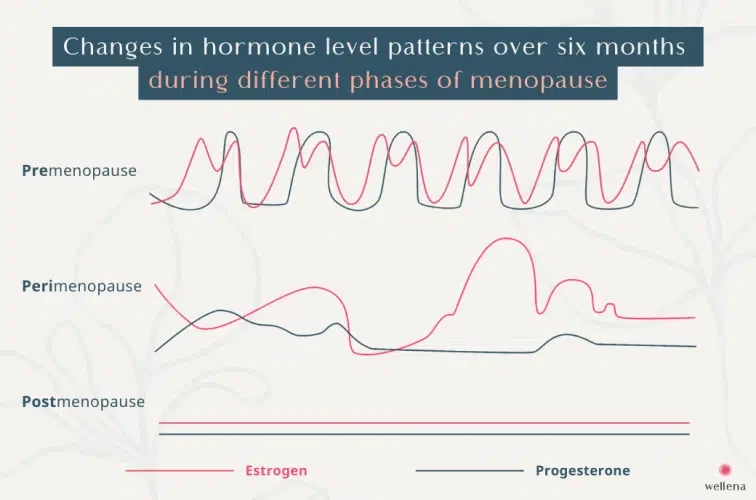
It’s not defined by a sudden drop in hormones, but by fluctuations in estrogen and progesterone from cycle to cycle.
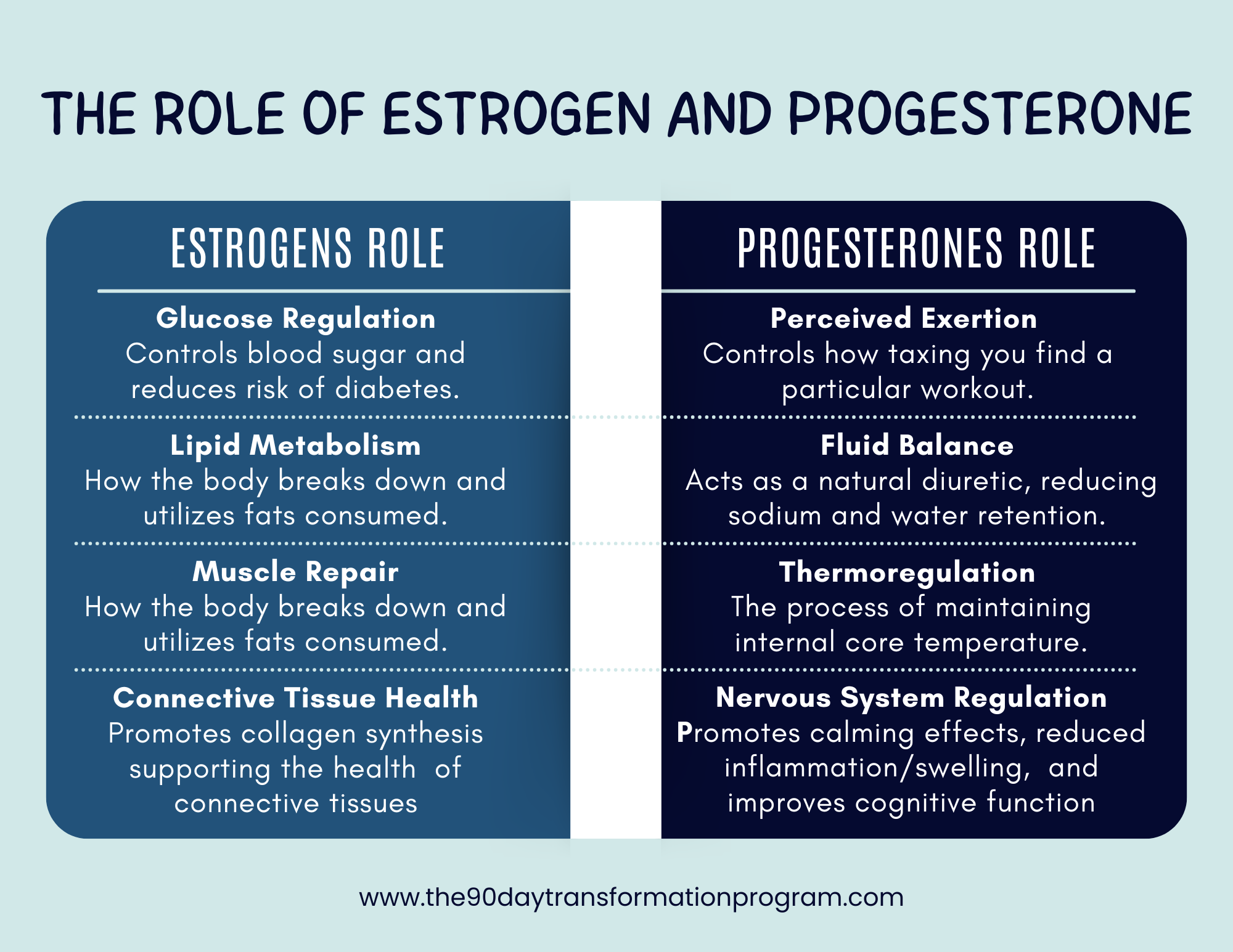
Remember the roles that estrogen and progesterone usually play in your body when stable.
Those regular hormone patterns start to change in perimenopause. These fluctuations influence:
Glucose regulation
Fat metabolism and distribution
Muscle repair and recovery
Nervous system regulation
The result is often less predictable energy, recovery, and training tolerance.
Why Your Body May Start Responding Differently
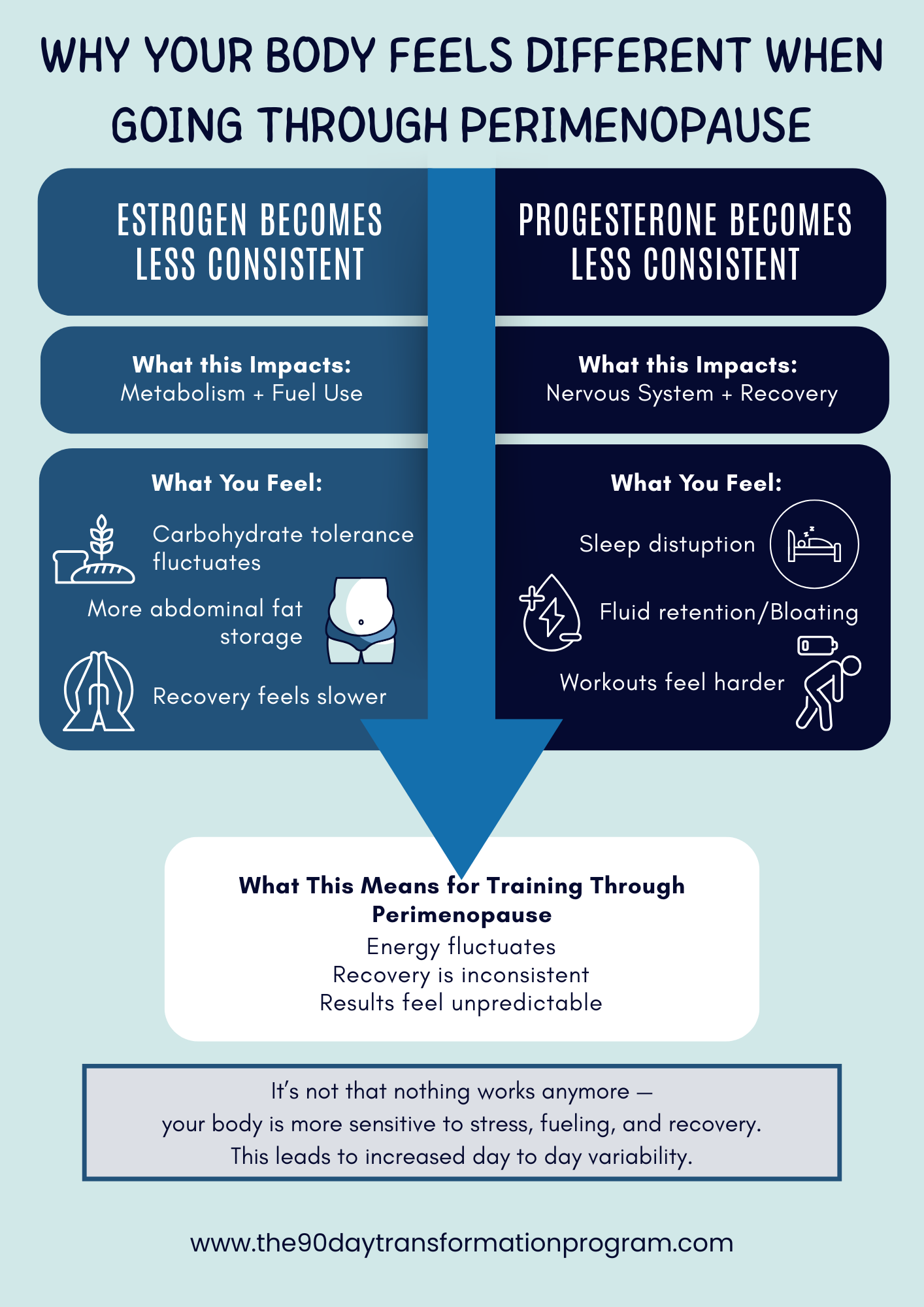
Estrogen plays a key role in insulin sensitivity and fat metabolism. As its signaling becomes inconsistent:
Carbohydrate tolerance may vary day to day.
Fat storage may shift more toward the abdomen.
Training may feel harder to recover from.
Research shows that women can experience an increase in central (abdominal) fat of ~4–7% across the menopausal transition, even without major weight gain (Lovejoy et al., 2008).
At the same time, progesterone variability can impact:
Sleep quality.
Fluid balance.
Perceived effort during workouts.
This often creates the feeling that “nothing works anymore”—when in reality, the body is more responsive to stress (both good and bad).
Stress Tolerance Becomes More Limited
This phase of life rarely happens in isolation.
Perimenopause often overlaps with:
Increased life and career stress.
Caregiving responsibilities.
Accumulated sleep disruption.
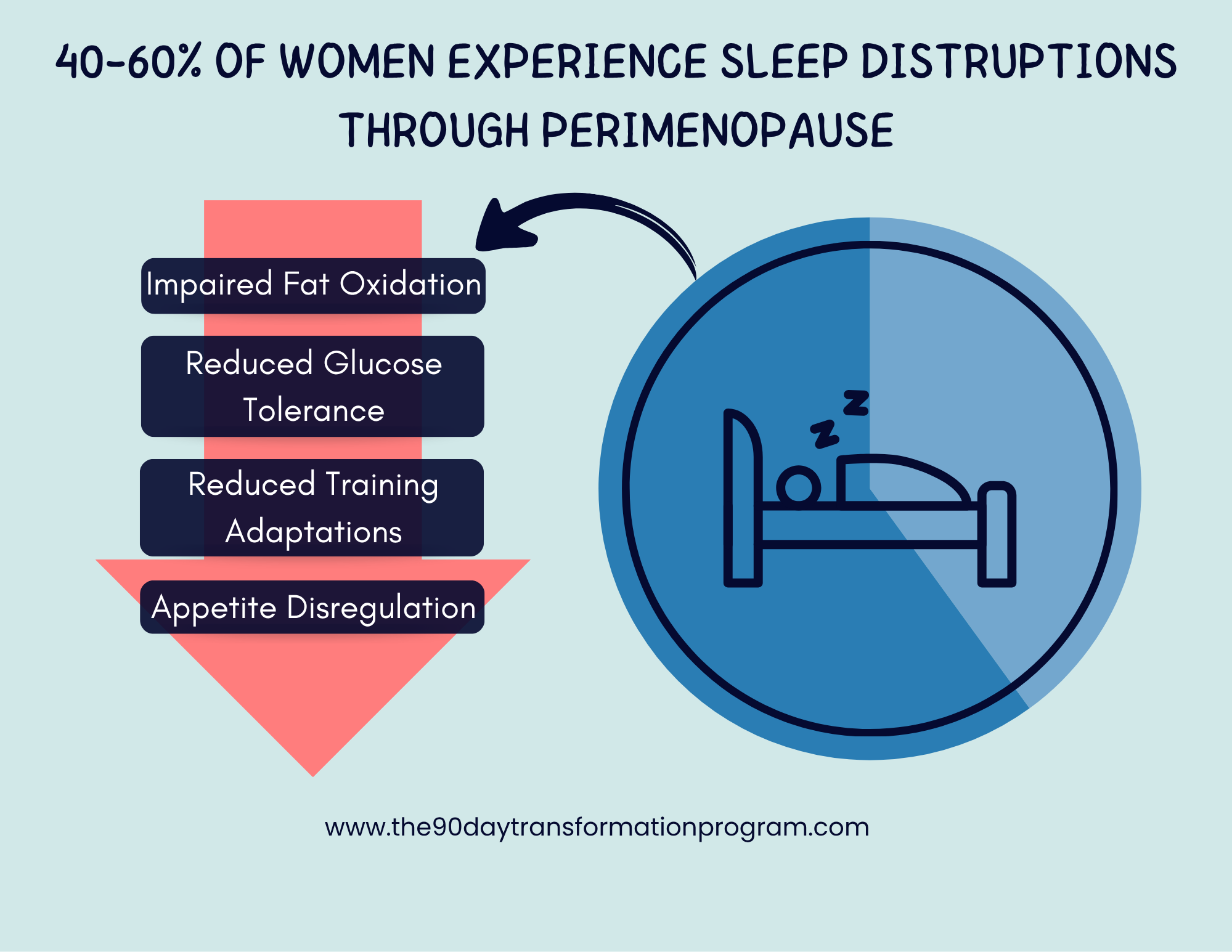
Sleep disturbances affect 40–60% of women during perimenopause, which alone can impair recovery, insulin sensitivity, and appetite regulation (Baker et al., 2018).
When combined with hormonal variability, the gap between productive stress and excessive stress narrows significantly.
Read More: Sleep, Stress, and Female Metabolism
Muscle Becomes Your Anchor
As hormonal signaling becomes less predictable, muscle becomes protective.
Maintaining lean mass supports:
Glucose control
Metabolic rate
Strength and independence
Bone health
From around age 30, adults lose ~3–8% of muscle mass per decade, with accelerated loss during menopause if not addressed (Mitchell et al., 2012).
More importantly—this is modifiable.

In a controlled trial, Miriam T. Nelson and colleagues showed that postmenopausal women who performed resistance training 2–3x per week significantly increased strength and preserved bone density, compared to non-training controls (Nelson et al., 1994).
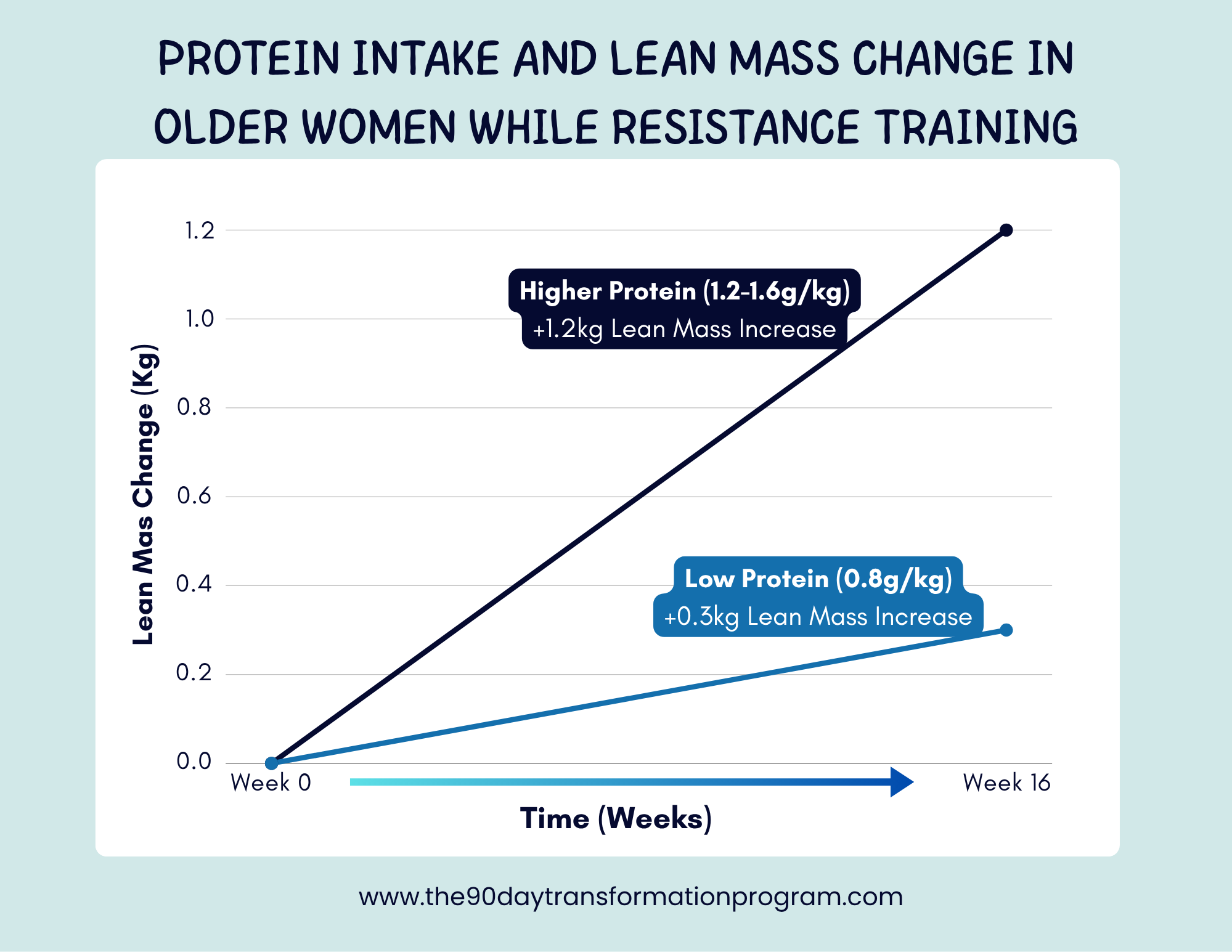
Similarly, a study by Wayne W. Campbell found that higher protein intake (~1.2–1.6 g/kg/day) combined with resistance training improved lean mass retention and metabolic health in older women, compared to lower protein intakes (Campbell et al., 2018).
Unlike fat loss strategies, strength training is a stable, predictable stimulus—making it one of the most powerful tools during this phase.
Read More: Why Building Muscle Is A Non-Negotiable For Women After 30
Why Dieting Often Backfires
One of the most common responses to these changes is increased restriction.
But during perimenopause, aggressive dieting often creates more problems than it solves.
Chronic under-fueling can:
Increase stress hormone activity
Worsen fat distribution
Impair recovery and sleep
Reduce muscle preservation
Instead of accelerating fat loss, it often leads to plateaus, fatigue, and regression.
Read More: Why Chronic Dieting Backfires in Women after 30
A More Effective Approach

Rather than restriction, nutrition during this phase benefits from a focus on adequacy:
Protein to preserve muscle
Carbohydrates to support training and nervous system function
Sufficient energy intake to stabilize physiology
Recovery becomes equally important:
Smarter programming (not just harder training)
Adequate rest between sessions
Prioritizing sleep quality
The Bigger Picture
Perimenopause isn’t a loss of capability—it’s a shift in physiological sensitivity.
When training, nutrition, and recovery are aligned with that reality, progress doesn’t stop—it becomes more consistent and sustainable.
This phase isn’t about doing more.
It’s about doing what matters—better.
References
Baker, F. C. et al. (2018). Sleep problems during the menopausal transition. Sleep Medicine Clinics.
Campbell, W. W. et al. (2018). Protein intake and muscle health in aging populations. Nutrients.
Lovejoy, J. C. et al. (2008). Increased visceral fat and decreased energy expenditure during the menopausal transition. International Journal of Obesity.
Mitchell, W. K. et al. (2012). Sarcopenia and age-related muscle loss. Journal of Applied Physiology.
Nelson, M. E. et al. (1994). Effects of high-intensity strength training on multiple risk factors for osteoporotic fractures. JAMA.